Opinion – Jan Kuitenbrouwer & Peter Vasterman
Transgender care The demand for transgender care is increasing rapidly. The originally Dutch treatment with puberty inhibitors is increasingly coming under international fire.
JAN KUITENBROUWER & PETER VASTERMAN – 30 December 2022 – https://www.nrc.nl/
ENGLISH TRANSLATION OF ARTICLE
‘Waiting lists for transgender care too long: ‘It will destroy you’”, was the headline of RTL News at the beginning of this year. Dutch gender clinics are overwhelmed by an almost exponentially growing demand for gender care. The previous cabinet installed a ‘quartermaster’ to initiate a drastic expansion of capacity. But: what kind of care should that actually be?
Until 2010 , an average of about 200 patients per year reported to a gender clinic in the Netherlands, including about 60 children and young people. Around 2013, the number of registrations suddenly doubles and from that moment the line goes up steeply. In 2022, there will be almost 6,000 people on the waiting list and more than 5,000 in treatment, including about 1,600 minors. The growth is also enormous in that group, there are also another 1,800 on the waiting list. They ‘do not feel at home in their own gender’ and want to be ‘in transition’. This growth trend is international. Underage patients at the British gender clinic Tavistock: from 51 in 2009 to 3,585 in 2022. Thousands of children were also on waiting lists there this year .
Feeling out of place in one’s own gender is called ‘gender dysphoria’ and nowadays often also ‘gender incongruity’. The treatment is largely based on the administration of ‘cross-sex hormones’, women receive testosterone to become more ‘masculine’, men estrogen to become more ‘feminine’. Teenage patients also use ‘puberty inhibitors’, substances that stop the physical process of puberty. Normally boys develop a low voice, beard and Adam’s apple, girls develop breasts, wider hips and ‘curves’. That process is stopped, the
‘secondary sexual characteristics’ do not form, time is gained for the child to explore his ‘gender identity’. Puberty inhibitors are a ‘pause button’. Should the need for transition disappear, the treatment will be stopped and puberty will still start, without adverse consequences, is the promise. Will the transition continue?
This approach was developed in the 1990s in the gender clinic of the VU Hospital (nowadays the Knowledge and Care Center for Gender Dysphoria of the Amsterdam UMC). In 2006, strict criteria were formulated in a study sponsored by hormone producer Ferring : there had to be gender dysphoria from an early age, which also worsens at the start of puberty; the patient is psychologically stable and receives sufficient emotional support. Possible side effects were not taken lightly, they were outweighed by the major benefits: relief from the torment called gender dysphoria. The approach really took off and in a few years it became ‘ Dutch Protocol‘ the international standard of care in this field. It is believed that many tens of thousands of children have been treated in this way all over the world. It is estimated – there are no official figures – that there are about 500 to 1,000 .
Being something different
This is a new type of patient. Before this boom, the typical ‘transsexual’ was an adult man, but the major growth is now among young people, especially girls (75 percent). They often do not present until puberty has already started, and they often have no history of gender dysphoria. In fact, even when they report this is often not really the case, they claim gender incongruity, they don’t suffer so much from it, they want to be something else. It is not a disorder, but an ‘identity’. What is striking is that many of these young people have additional psychological complaints, there are unprocessed traumas or they are struggling with their sexuality. One in four has an autism spectrum disorder. Are these complaints the result of their dysphoria or the cause? What should you treat?
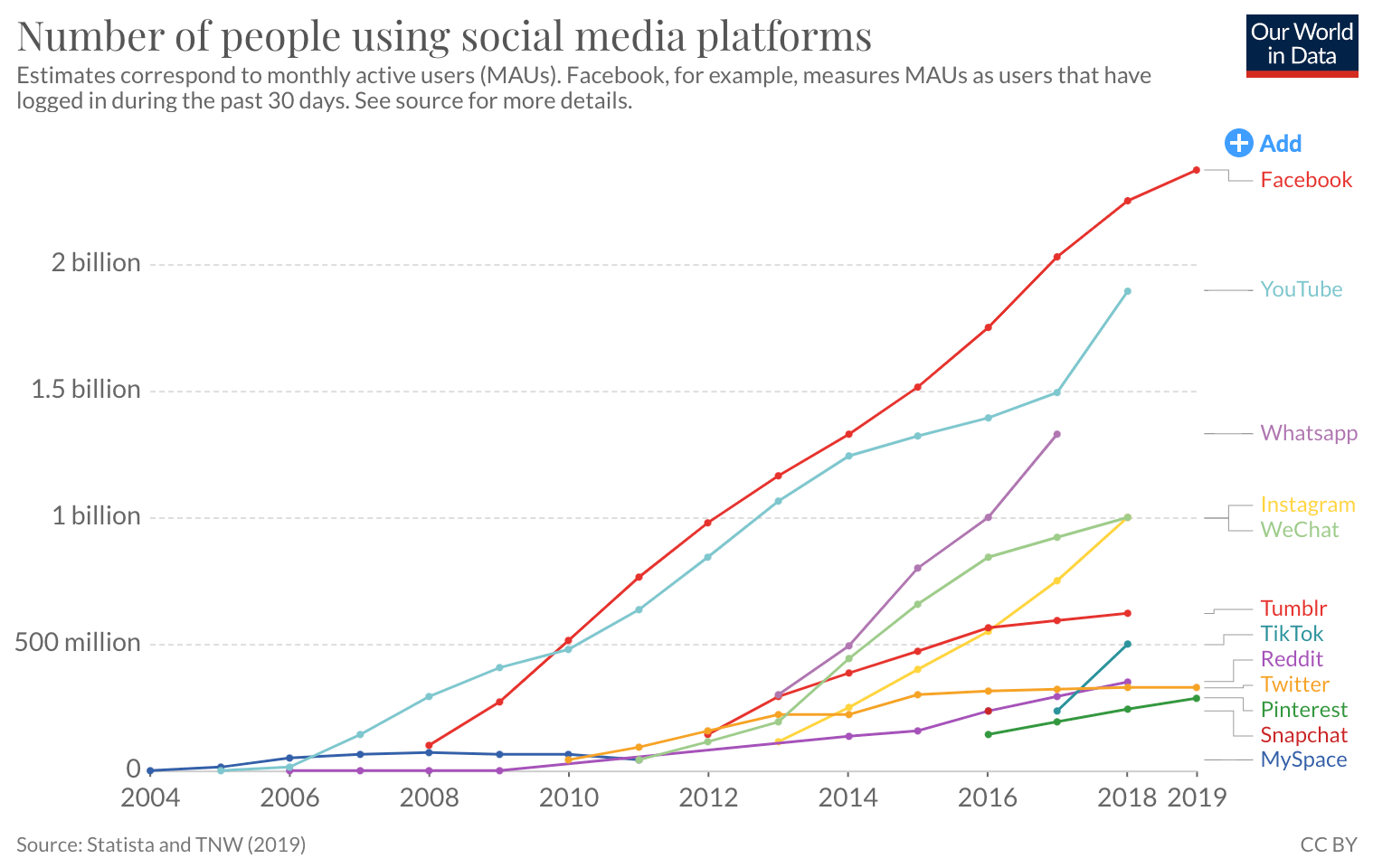
This boom is explained by trans organizations as the result of increased societal acceptance of gender diversity; doubters come out of the closet more easily. Critics point out that social acceptance of deviant behavior is slow to change, while this is a very abrupt , exponential growth that started around 2013. What happened then? Is it a coincidence that this explosion coincided with the spectacular growth of social media around the same time? The statistics show a striking resemblance. And if this has to do with social acceptance, then why mainly girls, while girls traditionally get more room for gender nonconformity than boys? In addition, also in the Netherlands, more and more people with regrets are manifesting themselves, who believe that they have wrongly been subjected to this irreversible treatment. They feel pushed and insufficiently protected against themselves.
{kind=link}
See the reasons why the Dutch protocol is being viewed more and more critically worldwide . Is it the right approach for this new group? And is it as safe and effective as long assumed? The answers are disturbing. Following extensive scientific evaluations of the treatment, health authorities in Sweden , Finland and the United Kingdom have recently decided to emphasize psychological treatment in children and to prescribe puberty inhibitors only in very severe cases or, as in Florida, even completely . to stop .
According to the Swedish review (2021), the available data are not sufficient to properly assess the effects on gender dysphoria, psychosocial conditions, cognitive functioning, and physical health. “The risks currently do not outweigh the possible benefits,” says the Swedish health authority. The Finnish report (2020) comes to a similar conclusion, as does the British ‘Cass Review’ (2022). The leading British pediatrician Hilary Cass condemned the British application of the Dutch protocol and, based on her report, the Tavistock gender clinic, the largest in the world, was immediately closed ….